Date: April 5, 2018
DOI: 10.4103/0971-3026.155882
Indian Journal of Radiology and Imaging / May 2015 / Vol 25 / Issue 2 203
Real-time ultrasound: Key factor in identifying celiac artery compression syndrome
Raina Anil Tembey, Aneeta S Bajaj, Prasad K Wagle1, Abdul Samad Ansari2
Departments of Radiology and Imaging, 1Surgery and 2Critical Care Medicine, Lilavati Hospital and Research Centre, Mumbai, Maharashtra, India
Abstract:
The median arcuate ligament syndrome (MALS) or celiac artery compression syndrome (CACS) is a rare entity, presenting clinically with postprandial abdominal pain and weight loss. The diagnosis is made on computed tomography (CT) angiography, which reveals extrinsic compression of the proximal part of the celiac artery by the median arcuate ligament, producing a characteristic hooked appearance. We report a case of the celiac artery compression syndrome, diagnosed by Doppler USG evaluation
Introduction:
The median arcuate ligament syndrome (MALS) or celiac artery compression syndrome (CACS), is a rare condition, classically presenting with chronic postprandial abdominal pain, weight loss, and epigastric bruit. The pathophysiology is explained by either compression of the splanchnic nerve plexus causing neurogenic pain or compression of the proximal celiac trunk by the median arcuate ligament (ventral arch of the aortic hiatus, formed by tendinous fibers between both the diaphragmatic cruras) causing chronic mesenteric ischemia.[1] The incidence of this syndrome is reported to be between 1.76-4%.[2]
Case Report:
A 27-year-old female patient presented with a one-year history of postprandial abdominal pain and weight loss.
Her clinical and laboratory investigations did not reveal any significant abnormality. An USG examination of the abdomen done previously had not detected any pathology. In view of the unexplained abdominal complaints and weight loss, a CT (SOMATOM Definition Flash 128 slice dual source CT Scanner, manufactured by Siemens in Germany) scan of the abdomen and pelvis was advised. The CT identified a narrowing at the level of celiac artery origin, without any post stenotic dilatation [Figure 1]. No atherosclerotic changes were observed in the aorta or any of its major branches. A Doppler USG was suggested to assess the hemodynamic significance of the narrowing. Real‑time Doppler USG was first performed in a fasting status. The celiac artery flow velocities were examined in the supine and erect position and the angle between the celiac trunk and aorta was measured. The angle between the celiac trunk and aorta was 52.5° [Figure 2]. The celiac artery appeared narrowed at its origin and showed a turbulent flow [Figure 3A]. The peak systolic and end diastolic velocities in the supine position, at inspiration, were 201 and 61 cm/second [Figure 3B]. The peak systolic and end-diastolic velocities in the supine position, at expiration, were 323 and 136 cm/second [Figure 3C]. The peak systolic and end-diastolic velocities in the erect position were 99 and 35 cm/second [Figure 3D]. The elevated velocities in the supine position, at expiration, were reduced in the erect position. Also, the narrowed lumen of the celiac artery origin, in the supine position [Figure 4A], was reversed to a normal caliber in the erect position, with a more vertical orientation of the celiac axis [Figure 4B]. These findings raised a possibility of CACS. The aorta and superior mesenteric artery showed a normal B mode and Doppler findings.

Figure 1: Sagittal CT image shows focal narrowing at the origin of celiac artery

Figure 2: The angle between the celiac trunk and aorta is 52.5°
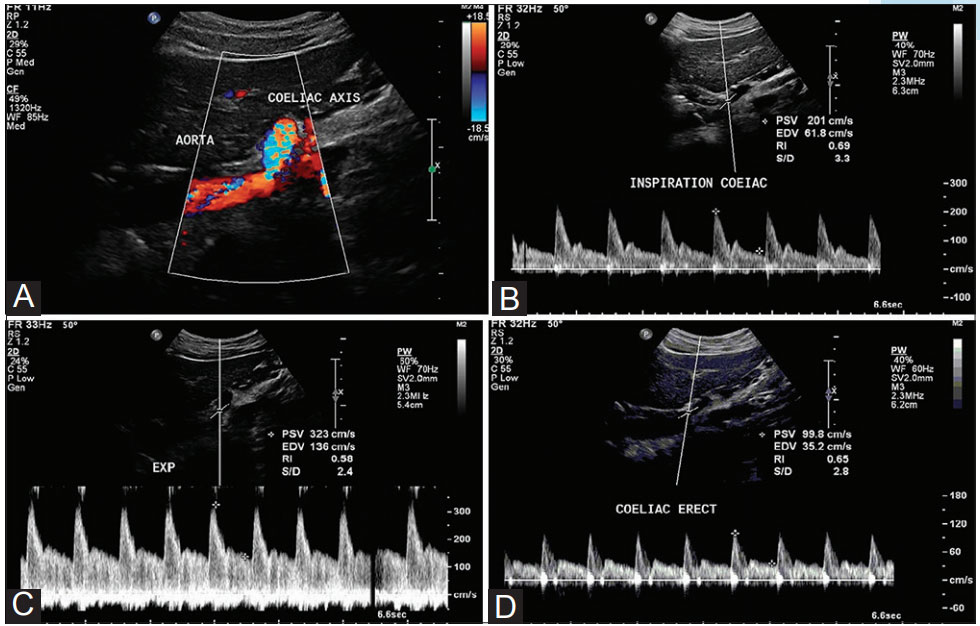
Figure 3 (A-D): (A) Color Doppler USG shows an aliasing artifact. Spectral Doppler USG taken on (B) inspiration and (C) expiration. Significantly elevated peak systolic velocity is seen on expiration. Spectral Doppler measurements in erect position (D) show normal peak systolic and end-diastolic velocities

Figure 4 ( A and B): (A) B mode USG in supine position shows narrow caliber of the celiac artery origin (B) B mode USG in erect position shows normal caliber of the celiac artery origin, with a more vertical position of the celiac axis
The patient underwent a laparotomy. At laparotomy, it was observed that the median arcuate ligament was causing compression of the celiac axis [Figure 5A]. The ligament was divided and secured [Figure 5B]. Post‑surgery, she has remained symptom‑free and a Doppler USG examination performed seven days after surgery did not reveal any elevated velocity at the celiac artery origin in the supine position, on expiration. The peak systolic and end-diastolic velocities of the celiac artery, on expiration, post surgery, measured 132 and 44 cm/second, respectively [Figure 6].

Figure 5 (A and B): (A) The red tape is holding the celiac axis below the ligament. The umbilical tape has the median arcuate ligament looped (B) The red tape is holding the celiac axis. The median arcuate ligament has been divided. The instrument shows the crus of diaphragm

Figure 6: Postoperative spectral Doppler USG reveals normal peak systolic and end diastolic velocities, even in the supine position, on expiration
Discussion:
The median arcuate ligament is a fibrous arch that unites the diaphragmatic crura on either side of the aortic hiatus. The ligament usually passes superior to the origin of celiac artery, however, in 10-24% of the subjects the ligament may cross anterior to the proximal portion of the celiac artery. It may then compress the celiac axis resulting in a compromised blood flow. Harjola was the first to describe the celiac artery compression syndrome, in 1963. It typically occurs in young patients (aged 20-40 years) and is more common in thin women. The affected individuals may complain of postprandial abdominal pain and weight loss. Abdominal auscultation may reveal a midepigastric bruit, varying with respiration. The diagnosis is confirmed by radiological investigations. The symptoms are probably due to compression of the celiac axis by the median arcuate ligament causing a compromised blood flow.[3]
Celiac artery compression may be investigated with the Doppler USG, MDCT angiography, selective catheter angiography, and magnetic resonance angiography. In patients with CACS, CT angiography demonstrates a characteristic focal narrowing in the proximal celiac axis. The focal narrowing has a characteristic hooked appearance, which can be useful in distinguishing this condition from other causes of celiac artery stenosis, such as, atherosclerosis. Post‑stenotic dilatation and collateral vascular vessels are among the features of CACS.[4] The CT scan of our patient showed luminal narrowing at the origin of celiac artery. However, there was no post-stenotic dilatation seen.
Gruber et al., in their study on the comparison between CACS patient and healthy volunteers, stated that functional USG imaging may be the best diagnostic option to define subjects with an acceptably high probability of suffering from CACS - the combination of a maximum expiratory peak velocity of >350 cm/second and a deflection angle higher than 50°.[5] In our patient the maximum expiratory peak systolic velocity was 323 cm/second and the deflection angle was 52.5°
Wolfman et al. suggested that the celiac artery should be investigated not only in full inspiration and expiration, but also with the patient in the erect position. Abnormal findings with CACS revert to normal during inspiration, as the celiac artery descends into the abdominal cavity during inspiration. This results in a more vertical orientation of the celiac artery, which often relieves the compression. With the patient in an erect position, the celiac artery descends further into the abdominal cavity, resulting in an even more vertical orientation, and as a result, the ligament relieves of compression.[3] Our patient showed a narrowing at the origin of celiac artery in the supine position. In the erect position the celiac artery origin showed a normal caliber and the celiac axis assumed a more vertical orientation.
Ozel et al., in their study of ultrasonographic diagnosis of the median arcuate ligament syndrome - a report of two cases - observed that in one of their cases, the peak systolic velocity at the celiac trunk was elevated in expiration. The velocity reduced during inspiration, but was still high. Re-examining the patient in an erect position revealed that the peak systolic velocity was in the normal range.[6] In our case also, even though the peak systolic velocity of celiac artery reduced in inspiration, as compared to expiration, it was still in the higher range. However, the peak systolic velocity measurement in the erect position was within the normal range.
Our case, thus illustrates the contribution of the Doppler in elucidating the hemodynamic significance of the celiac artery narrowing seen on CT. Dynamic evaluation demonstrated that the elevated velocity at the compressed segment of the celiac artery on expiration in the supine position returned to normal values in the erect position. Afollow‑up Doppler performed after division of the median arcuate ligament showed reversal of the hemodynamic changes.
References:
- Chaiwatcharayut W, Lekah A, Kurklinsky A. Celiacomesenteric trunk as a cause of median arcuate ligament syndrome. J Med Ultrasound 2013;21:39-42.
- Göya C, Hamidi C, Hattapoğlu S, Çetinçakmak MG, Teke M, Kuday S. Diagnosis of median arcuate ligament syndrome on multidetector computed tomography. J Med Cases 2013;4:616-9.
- Chou SQ, Kwok KY, Wong LS, Fung DH, Wong WK. Imaging features of median arcuate ligament syndrome. J Hong Kong Col Radiol 2010;13:101-3.
- Karahan OI, Kahriman G, Yikilmaz A, Ok E. Celiac artery compression syndrome: Diagnosis with multislice CT. Diagn Interv Radiol 2007;13:90-3.
- Gruber H, Loizides A, Peer S, Gruber I. Ultrasound of the median arcuate ligament syndrome: A new approach to diagnosis. Med Ultrason 2012;14:5-9.
- Ozel A, Toksoy G, Ozdogan O, Mahmutoglu AS, Karpat Z. Ultrasonographic diagnosis of median arcuate ligament syndrome: A report of two cases. Med Ultrason 2012;14:154-7.